Silver here. First Amendment badass Marc Randazza posted a tweet with a curious graph. He wrote:
1) I dont know if this is fake
2) If it is not fake, what does this tell us?
It’s not a fake. I went to the CDC’s website and downloaded the same data, plotted it myself.
(Edited to add: I revised the chart to try to make it more legible.)
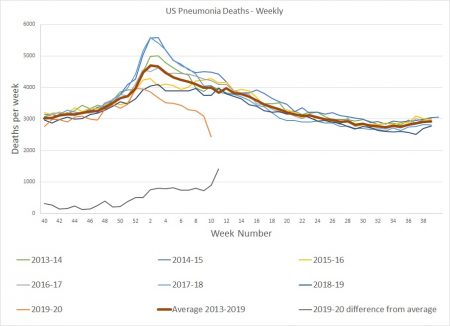
The traces for deaths attributed to pneumonia for the seven flu seasons (the CDC defines flu season as starting in week 40 each year) are straight from the CDC data. I added the heavier red trace “Average 2013-2019” and the lower trace “2020 Difference from average.” Any mistakes are mine.
Early in this season the pneumonia deaths were slightly less than the average from the previous years, but suddenly there was a significant drop. The last available week’s data shows a difference of about 1500 deaths per week compared to the average.
What does it mean? Thanks to some sleuthing by members of the forum, we know that revised CDC guidelines allow assigning “Covid-19” as cause of death without a confirming test.
A reasonable explanation is that some deaths formerly attributed to pneumonia are now being classified as caused by covid-19.
You are correct! This is a purposeful error being created by the powers that be to make the deaths from the Chinese Virus (CV)seem more scary than they really are. New York officials admitted that if a person has the CV but dies from other causes it is treated as a CV death. Similarly, if a person who has the CV dies and it is the result of the CV it is counted as a CV death. Italy is another entity that has overstated the numbers of people dying from the CV. Since Italy has allowed a mass Chinese migration to the Northern part of their country I would think they would want to show low numbers of people dying from the CV. The frustrating part of the whole issue is that once a person is buried you may not know if that person died of the CV or by natural causes. So how are we to know when this mystical peak everyone talks about flattens out for those who have “died” of the CV?
The people generating the models driving government actions are one of either three things;
1.) incompetent
2.) Promoting an agenda
3.) some of both of the other two
Comrade, what does the make the people who quote them?
An even more reasonable explanation is that, while some deaths maybe getting misclassified (we know it’s happened in the US, but so far have no idea how often), far more of them are not happening at all because everyone is at home hiding under their beds and therefor unable to get the flu in the first place.
“A reasonable explanation is that some deaths formerly attributed to pneumonia are now being classified as caused by covid-19.”
Not exactly.
Covid-19 generally causes death by (drum roll please) … pneumonia.
So there are a couple of plausible explanations.
One is that pneumonia deaths which previously were left unspecified as to cause, or were attributed to other causes, are being attributed to covid-19 specifically because that’s what’s going around and in the absence of available/reliable tests, why NOT pick the cause of death that’s most likely to bring some of Uncle Sugar’s money to your hospital from the buffet available?
Another is that COVID-19 is actually displacing other pneumonia-causing infections — killing the same people who would have been killed by those other infections, because it gets to them quicker and hits them harder than e.g. influenza..
It will be interesting to find out — if we ever DO find out — just how much over-diagnosis of COVID-19 was going on in the US during this time period. Various incentives, running the gamut from panic to government funding, guarantee that there’s at least SOME of that going on.
I haven’t seen any statistics showing what the death toll was this time last year. It would be interesting to find out that there wasn’t that much difference – or none at all.
Bob,
The statistics for pneumonia are shown in the chart, for last year and the 6 years before that.
Thomas,
I think we are saying the same thing using different words. Deaths that used to be classified as pneumonia are now classified as covid-19.
I didn’t speculate as to motivation. The causes you offer are certainly reasonable to consider.
But there’s another thing. As you point out, covid-19 causes death by pneumonia. Specifically, the virus attacks the mucous membranes in the lungs. The body’s immune system swiftly develops antibodies to the virus, and kills the infected cells.
But this leaves a lot of dead mucous membrane tissues. Bacteria settle in and cause pneumonia. The truly dangerous respiratory illness is the one where you get sick, get better, then suddenly get much worse. Rapid treatment with antibiotics can sometimes save the patient, but it’s safer to be under the doctor’s care before the emergency. This is why doctors will often prescribe antibiotics to patients with a viral respiratory disease – to treat the bacterial growth before it becomes lethal.
A careful determination of the cause of death would examine whether the death was due to overwhelming destruction of lung tissues by the coronavirus, which left the patient unable to take in sufficient oxygen to live, or if the death was caused by the secondary bacterial infection.
But that sort of careful work is specifically not required now, and we will never find out if or how much “over diagnosis” of covid-19 took place.
Silver,
I’m not saying that pneumonia deaths are irrelevant, I’m asking what the total death toll for all causes was during the same period last year.
Just waiting; the answer is #2
Just in, Methinks if this is true all I can say is; Boom!!!;
https://medium.com/@agaiziunas/covid-19-had-us-all-fooled-but-now-we-might-have-finally-found-its-secret-91182386efcb
Professor Silver please comment.
I just realized that the link does not work but I did post the article completely on Claire’s Cabal;
https://www.clairescabal.com/forum/index.php?topic=4737.0
Thank you for the links Comrade X.
This isn’t the first time that Medium has censored news and opinions that don’t match the official narrative of the day. I’m growing to distrust them.
If what the article says is true, it’s extremely interesting and probably very important. But there are no references, no links to sources, nothing. The long-winded explanation of respiration borders on condescending and obscures the central message. I will do my own research and try to corroborate this.
If this is accurate, it closely matches the fervent plea by an emergency medicine doctor that the high-pressure ventilator protocols currently in use are wrong.
https://www.youtube.com/watch?v=k9GYTc53r2o
https://www.youtube.com/watch?v=QWaq8HoEROU
He describes patients that are suffering from acute hypoxia rather than Acute Respiratory Distress Syndrome, ARDS. High pressure ventilation is used to treat ARDS as a result of respiratory failure. His covid-19 patients don’t have respiratory failure.
I’m just trying to be a good student!
Government smashed your small independent business, bans you from working, yet demands you still pay your bills.
2) If it is not fake, what does this tell us?
It’s just flu, and this is Kristallnacht for the entire lower-middle class, just with slightly different optics so you don’t recognize it.
Well, shit. Really.
How sewage could reveal true scale of coronavirus outbreak:
https://www.nature.com/articles/d41586-020-00973-x
Now that’s Twilight Zone stuff.
That’s fun stuff right there.
Also, if there’s evidence out in the world that this is in fact a new virus, I haven’t seen it. I’ve looked. How many people were tested for this virus last flu season? None, right? Okay then.
So many problems with all the data in all directions. False positive rate in testing? Which test? False negatives? Which population was sampled prior to the last few months? Does “flattening the curve,” even if it works, actually reduce deaths? Does a quarantine of healthy people work? Has it ever? Since it hasn’t, why is this case different? The problems with the mainstream crap go on and on.
I come from a software/security/risk-assessment sort of world. None of what’s going on, meaning the so-called decision-making, makes any sense to me.
Actually…I take that back. It all makes sense. It’s just annoying. Politicians have to do something or risk being considered responsible for whatever happens. Whatever they do, regardless of the result, they’re held blameless bc “at least they tried!”
Oh, for a world where the idea of letting that kind of blowhard decide to “do something” that affects others, and then going along with the nonsense, would be greeted with the derision it deserves.
Maybe someday. Meanwhile: same old, same old.
Comrade X
I’m going with Door # 3.
Does “flattening the curve,” even if it works, actually reduce deaths?
It can. Slowing the spread of a disease to the point where medical facilities can keep up with serious cases will save lives, since people who need treatment will get it. You don’t have to triage.
However, flattening the curve to the point where, as in my county, no one is catching it means that no one gains immunity until a vaccine is invented, tested, produced, distributed, and used to inoculate 300,000,000 people. By which time the lockdown will have cost far more lives than Covid.
Our local Meals on Wheels program distributes hundreds of meals per day (in a town of 25,000) to people who can’t get out, and who now can’t have visitors. MoW used to deliver every day, but to “cut exposure” they’ve gone to two deliveries a week, one hot meal and making up the rest with frozen or shelf-stable meals. They are phoning each client every day to check up, but other than that, many of these elderly or disabled people are essentially in solitary confinement.
It’s at least as likely that flattening the curve would cost lives. A short-duration shock to the hospital system would undoubtedly result in deaths. However, deaths due to a longer-term crippling of that system might be greater in number. Other unintended consequences of the shutdowns, also.
But there are even worse ideas out there. Vaccination passports? Maybe:
https://mobile.twitter.com/FatEmperor/status/1247509531627749377?s=20
Makes me think about covid parties. Like for chickenpox. And not wearing a mask, except for maybe a bandana when entering a bank. Fashion still counts for something.
Another explanation for the apparent drop in flu deaths is that… it’s only apparent and due to a data collection lag that is ordinary and in-line with previous years. See https://twitter.com/TylerMorganMe/status/1247706877145776129
Reference Comrade X’s link:
https://hotair.com/archives/allahpundit/2020/04/08/attention-medical-professionals-might-not-need-ventilators-coronavirus-patients/
With ventilators running out, doctors say the machines are overused for Covid-19
Totally unrelated: We publish a weekly “Teacher Feature” outlining a local schoolteacher. The interview I did this morning was a young lady who graduated high school in 2015.
[sigh]
IMHO the overuse of ventilators today is akin to the overuse of leeches in the yesterday.
“IMHO the overuse of ventilators today is akin to the overuse of leeches in the yesterday.” Or worse yet, as in George Washington’s case, blood letting: https://jeffreydachmd.com/2013/04/donating-blood-prevents-heart-disease/
Just in today. Antibody testing in Santa Clara: infection rate 50-85x the known cases. Puts fatalities in line with seasonal flu. Maybe very slightly higher. Maybe lower.
https://www.medrxiv.org/content/10.1101/2020.03.24.20043067v1.full.pdf
The linked paper doesn’t say that. Here’s the second sentence: “In the absence of wide-spread testing, we provide one approach to infer prevalence based on the assumption that the fraction of true infections needing hospitalization is fixed and that all hospitalized cases of COVID-19 in Santa Clara are identified.”
In other words, they’re making a guess since there _isn’t_ testing. Fatalities aren’t mentioned at all.
They tested 3300+ people. It’s the best data we have. One of the authors was John Ioannidis.
There is a difference between raw information and its interpretation.
This paper didn’t mention fatalities bc they weren’t involved in measuring those. However, that doesn’t mean we can’t look them up. And calculate.
The main point here is that the number of (known) cases is clearly known & so is the number of fatalities ascribed to the virus. And the case fatality rate estimates have been quite high. Calculations and further reading are not difficult.
A large question that’s been lurking all along is: what’s the actual infection fatality rate? To know that, you need to know how many are infected in the first place. That number is what needs testing. This was a bunch of tests. In line with the Diamond Princess cruise ship numbers too, if you’d like to check Ioannidis’s “evidence fiasco” paper.
To refer to this as a guess is…um. Well, it’s what it is. Could be there’s a real problem with the antibody test. Could be there isn’t.
Another paper with a similar result, which admittedly strikes me as much more guesslike:
https://www.medrxiv.org/content/10.1101/2020.04.01.20050542v2
Or a Danish blood donor study, again with a similar result:
https://www.rt.com/news/486017-denmark-covid19-mortality-study/amp/#click=https://t.co/Jkcf3nnle3
But the point I was making is that the original study I cited (which consists of 3300+ of the very tests I think we would agree are needed) showed, as I said, a 50-85x greater number of infections than previously reported. Which is great news re: mortality. Even if they didn’t explicitly identify the implications.
I’m beginning to suspect that you may have simply linked to the wrong paper by mistake. The one you linked to is about estimating infection rates based on hospitalization. It has nothing to do with actual testing. Also, you said “just in today,” but the date in the linked paper’s URL and the most recent data contained in it suggest it’s from March 24. Perhaps you should double-check the paper you linked to and confirm that there’s no copy/paste error here?
Holy…uh…crud. Yes, that was the wrong link. Second time I’ve done that today. Fortunately I only sent the first one to my mom.
https://www.medrxiv.org/content/10.1101/2020.04.14.20062463v1
Though the other was interesting also.
Sorry.
Dr. Ioannidis, one of the authors of that study, gave an interview where he talked about it:
https://www.youtube.com/watch?v=cwPqmLoZA4s